|
Psychology and Psychotechnics
Reference:
Bochkina E.V., Doronicheva M.M., Shatilova N.N., Plokhikh D.A.
Varieties of Comorbid Disorders in Children with Mental Retardation
// Psychology and Psychotechnics.
2022. ą 4.
P. 1-13.
DOI: 10.7256/2454-0722.2022.4.38812 EDN: OKFMMJ URL: https://en.nbpublish.com/library_read_article.php?id=38812
Varieties of Comorbid Disorders in Children with Mental Retardation
Bochkina Elena Valeryevna
ORCID: 0000-0003-1099-0047
Lecturer Moscow Financial-Industrial University "Synergy"
143530, Russia, Moscow region, Dedovsk, Voykova str., 14

|
bochkina.elena@gmail.com
|
|
 |
Other publications by this author
|
|
Doronicheva Mariya Mikhailovna
Neurologist, Pediatric Psychoneurology Research Center
74 Michurinsky Ave., Moscow, 119602, Russia
|
|
maridoro@mail.ru
|
|
 |
Shatilova Nadezhda Nikolaevna
PhD in Medicine
Neurologist, Pediatric Psychoneurology Research Center
74 Michurinsky Ave., Moscow, 119602, Russia
|
|
shatilovaN@mail.ru
|
|
 |
|
Plokhikh Dmitrii Aleksandrovich
PhD in Medicine
Deputy Chief Physician for Educational and Methodological Affairs, Kuzbass Regional Children's Clinical Hospital named after Yu.
650029, Russia, Kemerovo, Voroshilova str., 22a
|
|
d.plokhikh@rambler.ru
|
|
|
|
DOI: 10.7256/2454-0722.2022.4.38812
EDN: OKFMMJ
Received:
21-09-2022
Published:
30-12-2022
Abstract:
The subject of the study is comorbid disorders of children with mental retardation. The object of the study is the frequency of comorbid disorders of the children with mental retardation. Using a retrospective analysis of medical records, the authors examine in detail the neuropsychiatric manifestations and behavioral stereotypes that frequently occur in the study sample of children. These behavioral stereotypes or comorbid disorders were noted by parents or health care professionals who interacted with the children. The total sample included 1,000 preschool and young children (from 1.5 to 7 years old) with various neuropsychiatric speech diagnoses - delayed speech development, autism spectrum disorders, delayed psycho speech development, and other unspecified speech diagnoses. The main finding of this study is that a list of the most common comorbid disorders was compiled. Using this list of the most common behavioral disorders, it is possible to make a screening assessment of mental development and identify the degree of its delay on the basis of the formed behavioral and speech patterns. This will help specialists (psychologists, speech therapists, defectologists and neuropsychologists) working with children to provide them with the necessary assistance in a timely manner. The scientific novelty of the study lies in the fact that previously no comprehensive list of the most common behavioral disorders of the children with mental retardation was compiled. This list made it possible to differentiate the primary diagnosed child into one or another group according to the belonging to the diagnosis, with subsequent more thorough verification of the diagnosis.
Keywords:
autism spectrum disorder, delayed speech development, mental retardation, behavioral features, list of violations, primary diagnostics, behavioral disorders, behavioral stereotypes, speech disorders, assistance to a specialist
This article is automatically translated.
IntroductionEvery year there is an increasing number of children with impaired speech development. According to WHO, in the 2000s, every 6-1 child had a delay in speech development, now the data show that these developmental disorders are inherent in every 3rd child of preschool age. By school age, this indicator stands at 25% in Russia and 19% abroad [11, p. 170]. It is worth noting that the group of children with speech disorders includes not only those children with general speech underdevelopment, but also children with delayed speech development, autism spectrum disorder and children with combined diagnoses, one of the manifestations of which is delayed speech development. There are several generally accepted definitions for the term ZPR – foreign and domestic. In Australia and the USA, the ZPR is interpreted as ""auditory processing disorder"" [10, p. 34]. This definition is based on 44 different conditions identified in 2017, which manifest themselves in violation of the processing of audio stimuli by the cerebral cortex with absolutely preserved hearing. In the national science in 1959, G.E. Sukhareva proposed a definition of the concept of mental retardation (hereinafter referred to as PSR). By ZPR, the author understood mental retardation, in which the main higher mental functions (memory, thinking, imagination, attention, perception) are not so well developed compared to peers. The diagnosis of ZPR is made to a child in preschool and primary school age, if the signs of this diagnosis persist after 10 years, then the child is diagnosed with oligophrenia or infantilism. This definition was widely used in psychological, pedagogical and psychiatric literature until 1990. After 1997, it was expanded and supplemented with new diagnoses according to ICD - 10. These diagnoses included: 1. delayed speech development; 2. dyslexia; 3. dyscalculia; 4. alalia; 5. dysgraphy; 6. behavioral spectrum disorders (more recently, this includes ADHD); 7. enuresis; 8. encopresis; 9. speech disorders of various types; 10. ticks; 11. phobias; 12. unspecified, borderline diagnoses. This clinical diversity of children with ZPR is due to the fact that the damage to the nervous system is in different localization. Most of the clinical disorders can be correlated with the structural and functional model of the brain, which was developed by A.R. Luria. In this model, three structural and functional blocks of the brain were identified: "a) an energy block, b) a block for receiving, processing and storing extraceptive information, c) a block for programming, regulation and control of complex forms of activity" [9, p. 182]. The first block (energy) provides an optimal level of mental activity and a balance between the processes of arousal and inhibition. This block is located — from the brain stem to the mediobasal parts to the temporal and frontal lobes of the brain. Most children with ADHD have disorders and lesions in these areas. The second structural and functional unit is responsible for the main analyzer systems - skin–kinesthetic, auditory and visual. It is located "in the occipital and parietal regions, covering the associative zone and its overlaps (TRO)" [9, p. 183]. Due to the properly organized functioning of these areas, the memory and attention block is provided with information that the brain has previously perceived, processed and appropriated. Also, this unit is responsible for the implementation of optical-spatial activity and the arbitrariness of movements. That is why the majority of children with ZPR have violations in spatial-temporal orientation and pronounced stereotypical voluntary motor actions. The role of the third block is to organize the structural regulation and organization of the child's mental activity. This block is located in the frontal lobes of the brain. A.R. Luria noted that the work of the structures of this block is responsible for the proper functioning of such mental functions as forecasting (or building an anticipatory image according to E.V. Bochkina and I.B. Shiyan), goal setting, arbitrary attention, higher mental emotions, arbitrary memorization, mental and speech processes. All components of the structural and functional blocks of the brain are represented in it symmetrically in both hemispheres (right and left). The coordinated work of all three blocks in the two hemispheres of the brain is capable of ensuring full-fledged integrative activity of the brain and mutual enrichment of all its departments and functional systems. If any department is damaged, then this can lead to a violation in one of the three blocks. In which of the blocks the lesion is located can be judged by the peculiarities of clinical and behavioral manifestations.
Attempts to systematize behavioral manifestations in children diagnosed with ZPR have been made repeatedly, but there is no generally accepted classification to date. This is due to the fact that these disorders are at the junction of many diseases and developmental disorders that occur in pediatric and neuropsychiatric practice. Speech is a key mental function in the process of emotional-volitional, behavioral, social and intellectual development of a child. The influence of speech development on the intellectual development of a preschool child has been studied by a number of domestic and foreign scientists (a number of domestic and foreign scientists have studied intellectual development (E.V. Bochkina, L.S. Vygotsky, B.V. Zeigarnik, K. Levin, J. Piaget, etc.). They noted that with the help of speech, a child can display images of the surrounding world formed in his psyche. J. Piaget wrote that speech has the function of expressing thoughts and emotions, the better it is developed, the faster his socialization and intellectual development takes place [12, p. 301]. Figure 1 shows a diagram of the social development of speech in preschool children. 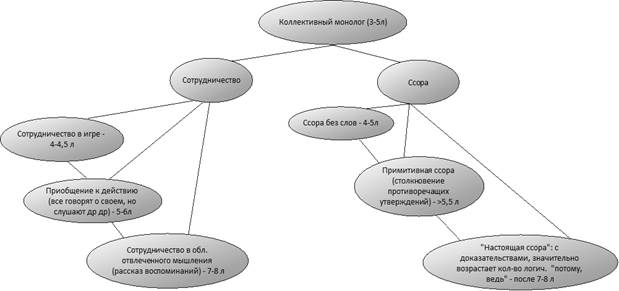
Fig.1 Socio-speech development of a preschool child In children with ASD, this path of social and speech development is distorted, because they hardly perceive the symbolic culture of the surrounding world and do not assign socially accepted norms of behavior and communication, and also experience difficulties in the process of spatial and temporal orientation in the surrounding world. In the works of B.V. Zeigarnik and K. Levin, it was noted that children suffering from speech or mental disorders have difficulties in the process of perception and orientation in the surrounding world [4;7]. L.S. Vygotsky noted that "a child with speech disorders also has disorders in mental development has difficulties in the process of perceiving sign-symbolic culture of the surrounding world" [3, p. 210]. E.V. Bochkina writes that "thanks to these images, the child shows us his level of actual mental development" [2, p.121]. When speech development is impaired, these images are impoverished and often not coherent, and "spatial-temporal representations are not formed or are not fully formed" [1, p. 95], notes E.V. Bochkina. N.S. Zhukova and K.S. Lebedinskaya identified the features of mental development in children with moderate and severe speech disorders. They attributed these features to: · spatial-temporal representations are violated, concepts for spatial orientation are difficult to differentiate; · low level of attention development, it is not stable; · broken images created in the imagination; · there are "stamped" actions in mental activity; · they get tired quickly and slowly get involved in the work; · the level of verbal memory development is reduced; · auditory perception is reduced. V.N. Zinovieva noted that "violations of speech development, as a primary defect, negatively affect the initially preserved intelligence" [5, p.114]. That is why violations in speech development entail violations in the mental development of the child. This type of disorders can include – a delay in intellectual development, a delay in the process of socialization and communication with peers and the occurrence of comorbid disorders. Behavioral or comorbid disorders are commonly understood as "stable changes in behavioral images that do not correspond to the norms of behavior accepted in society" [6, p. 87]. These behavioral disorders became the subject of our study. It should be noted that behavioral disorders in children with ASD were not a subject for independent research, because there was no complete classification of these manifestations. All available data in the psychological, pedagogical and psychiatric literature were reduced to 3-6 disparate behavioral manifestations, which did not always correspond to what the children demonstrated in the process of primary diagnosis. Recently, neurologists and psychiatrists, as well as specialists in psychological and pedagogical profile, have noted additional behavioral manifestations in children with ASD, which were not previously noted or were identified only in children with autism spectrum disorder or oligophrenia. This means that the clinical picture of these manifestations has expanded and requires significant improvement in accordance with the newly appeared data.
The theoretical analysis made it possible to identify a contradiction between the existing psychological, pedagogical and psychiatric needs in diagnostic lists that combine the most typical behavioral manifestations of children with ASD and their absence in specialists working with this category of children. Previously, there have already been attempts to systematize these behavioral manifestations, but there is no generally accepted classification today. Difficulties in the process of developing this list were caused by the fact that there is a clinical variety of manifestations of mental retardation, combined with delayed speech development and other neuropsychiatric diseases, such as autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD) and other unspecified diagnoses. These diagnoses have similar behavioral manifestations, but differ in the frequency of their manifestation. The objectives of our study were to identify behavioral features in children with delayed speech development (RR) and to compile a diagnostic list (quick diagnostic card) for a quick and high-quality primary diagnosis of a child with speech problems. Research methods: retrospective analysis of clinical data and a survey. These research methods were chosen in order to make the most complete collection of data obtained over several years of diagnostic work with children, because some children applied for primary diagnosis and diagnosis once and were no longer observed in a medical institution. Thanks to the survey, those behavioral manifestations that the child most often demonstrated at home and did not commit during the examination were revealed. A retrospective analysis of clinical data allowed us to supplement this picture with the manifestations that the child demonstrated during the initial examination. Research objectives: 1. conduct a retrospective analysis of medical records; 2. identify the main list of recurring behavioral disorders; 3. make a list of the most common comorbid disorders. The methodological basis of our research was: the cultural and historical theory of L.S. Vygotsky, which describes the stages of speech and intellectual development of preschool children (normotypic children and with special needs); the concept of intellectual development of Zh. Piaget, as a theory describing the nature of intellectual development of a preschool child; structural and functional model of the brain of A.R. Luria, describing the nature of the occurrence of the disorder according to the location of the lesion of the brain. Study participantsIn our study on the identification of behavioral features in children with speech development delay (SPD), 1,000 children aged 1.5 to 7 years from 2019 to 2022 took part. This group of children included 370 children with normal development and 630 children with delayed speech development. These features were identified using a retrospective analysis of the maps of children who had previously received rehabilitation or counseling from specialists of a neuropsychiatric hospital and a city polyclinic. At the moment, these children are not undergoing treatment and do not receive counseling. During data collection and analysis, all children were divided into several groups according to diagnosis and neuropsychiatric status. In total, we identified 4 groups of children. The first group included children with delayed speech development (hereinafter SRR); the second – children with delayed psycho-speech development (hereinafter SRR); the third group included children with autism spectrum disorder (hereinafter ASD); and the fourth group consisted of children with unspecified or combined diagnosis (these are those children who have there were signs of several diagnoses at the same time, for example, ADHD (attention deficit hyperactivity disorder) and ASD). It is important to note that all children included in the cohort sample were intellectually sound. The specifics of the distribution of children into groups are shown in Figure 2. 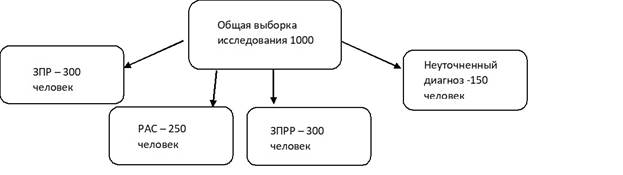
Fig. 2 Distribution of children in the study groups Research resultsBased on a retrospective analysis of medical records of children of early and preschool age (1.5 years – 7 years), it was revealed that most children of this age category with speech development delay have similar neuropsychiatric manifestations in behavior. These manifestations in some children were traced more clearly, in others, they did not occur regularly. Note that normotypic children may also exhibit these neuropsychiatric manifestations in behavior, but with a much lower frequency (1-2 manifestations in behavior). We attributed the following behavioral stereotypes to the identified neuropsychiatric manifestations: 1. Selectivity in food – a child may prefer to eat food of only one color or consistency. 2. Lack of control over the pelvic organs after 2.5-3 years.
3. The manifestation of instability of attention after 2 years, the child can hold his attention for no more than 2 minutes. 4. The child does not have an index gesture after 1.5 years. 5. The child does not react to the addressed speech – the child does not give any signs that he has heard a parent or a specialist when he is called by name or asked to do something (this does not manifest itself once). 6. Frequent manifestations of negativism - the child reacts with aggression to the addressed speech or requests (screaming, crying, biting or fighting). 7. Frequent waking up in a dream after 3 years - the child wakes up more than 3 times a night. 8. Manifestation of features of defecation (only standing or in diapers). 9. Babbling speech or bird language after 1.5 years. 10. Minimum vocabulary (50 words) after 3 years. 11. There is a sharp rollback in development after 1.5 -2 years - the child spoke words or sentences up to 1.5 years, and then abruptly fell silent (the same clinical picture is observed with other elements of intellectual development (the index gesture disappeared, stopped recognizing a significant adult, stopped pointing at objects, etc.)). 12. Fear of loud sounds – the child covers his ears if loud music is playing next to him, a dog is barking, fireworks are launched or someone is talking a little louder than usual (not shouting). These neuropsychiatric manifestations are reflected in the behavior of children in varying degrees of severity and combinativity in children with different diagnoses. So in children with ZPR, we noted from 3 to 5 manifestations. Most often it is selectivity in food, instability of attention and babbling speech or bird language after 1.5 years. There were from 4 to 7 manifestations in children with ZPRR. They had the same manifestations as children with ZPR, but several new ones were added to them: 1. selectivity in food; 2. minimum vocabulary after 3 years; 3. no pointing gesture after 1.5 years; 4. lack of control over the pelvic organs after 2.5- 3 years. In children with ASD from 6 and more. Negativism, manifestation of defecation features (only standing, in diapers, behind a curtain, etc.) and fear of loud sounds were often added to the above manifestations. Sometimes, this group of children had all 12 comorbid manifestations at once. In children from the latter group – with combined or unspecified diagnoses, there were from 3 to 7 comorbid manifestations. Most often, the following signs could be detected in them: 1. selectivity in food; 2. minimum vocabulary after 3 years; 3. the manifestation of instability of attention; 4. a sharp rollback in development after 1.5 years; 5. fear of loud sounds. Discussion of the results and conclusionAfter identifying comorbid manifestations in individual groups, we analyzed these indicators to identify the group most common in all the neuropsychiatric diagnoses we studied. The most common manifestations were attributed to us: 1. Selectivity in food. 2. The manifestation of instability of attention. 3. The child does not respond to the addressed speech. 4. Babbling speech or bird language after 1.5 years. 5. Minimum vocabulary (50 words) after 3 years. 6. There is a sharp rollback in development after 1.5 -2 years. 7. Lack of control over the pelvic organs after 2.5-3 years. These manifestations were noted in 75% of the examined children, and the first 5 of them? 87% of children of early and preschool age.
The obtained indicators give us the opportunity to compile a list of the most common comorbid disorders. This checklist can be used for screening assessment of the spectrum of comorbid disorders in a child with delayed speech development and to determine the direction of in-depth examination in connection with the prevailing behavioral pattern (ASD, delay of isolated speech, speech and cognitive development) and timely targeted correction. Belonging to a certain diagnosis can be revealed due to the number of behavioral behaviors present. The further direction for our research will be the work with these children on the development of the perception of the sign-symbolic culture of the surrounding world, through which socially accepted norms of behavior and communication are appropriated, and the development of spatial and temporal orientation in the surrounding world. Thanks to this work, we hope for the speech and intellectual development of this group of children, as well as the correction of these behavioral stereotypes by correcting their social communication and interaction skills.
References
1. Bochkina E. V. Features of the development of ideas about the cyclicity of space and time in children of senior preschool age / E. V. Bochkina // Psychology and Psychotechnics. − 2019. − ą 1. −Ń. 89-99. − DOI 10.7256/2454-0722.2019.1.28989.-EDN ZDVDOP.
2. Bochkina, E. V. Features of psycho-verbal development in preschool children with different types of brain tumors / E. V. Bochkina // International Journal of the Humanities and Natural Sciences.-2022.-ą 8-3(71).-Ń. 120-122.-DOI 10.24412/2500-1000-2022-8-3-120-122.-EDN WPAMZO.
3. Vygotsky L.S. History of the development of higher mental functions.-SPb: Peter, 2000.-400 ń. [Vygotsky L.S. History of the development of higher mental functions.-St. Petersburg: Peter, 2000.-400 p. (In Russ.)].
4. Zeigarnik B.V. Introduction to pathopsychology,-Moscow: Politizdat, 1982. [Zeigarnik B.V. Introduction to pathopsychology, Moscow: Politizdat, 1982. (In Russ.)].
5. Zinovieva V. N., Demidova A. P., Nesterova N. K. Peculiarities of psychological development of a child with severe speech disorders // Problems of modern pedagogical education. 2021. ą72-1.
6. Ermolenko E. N. Features of thinking in preschool children with a combined defect (cerebral palsy and mental retardation) / E. N. Ermolenko, V. S. Vasilyeva // Fundamental and Applied Science: collection of scientific articles on the results of research work in 2015.-Chelyabinsk: Chelyabinsk State Pedagogical Institute, 2015.-Ń. 86-90.-EDN UZUBFD.
7. Kovalevskaya, A. S. Changing the psychological and pedagogical status of autistic children / A. S. Kovalevskaya, I. N. Grebennikova // Motor activity in the formation of a lifestyle and professional development of a specialist in the field of physical culture and sports: a collection of materials of the X National Scientific and Practical conference with international participation dedicated to the 30th anniversary of the Faculty of Physical Culture of Novosibirsk State Pedagogical University, Novosibirsk, April 08, 2021. – Novosibirsk: Novosibirsk State Pedagogical University, 2021. – pp. 63-65. – EDN TQACDR.
8. Levin K. The field theory in the social sciences / [Per. E. Surpin].-SPb.: Rech, 2000.-200 ń. [Levin K. Field theory in the social sciences / [Per. E. Surpin].-St. Petersburg: Speech, 2000.-200 p. (In Russ.)].
9. Luria A.R. Fundamentals of Neuropsychology.-Moscow: Moscow University Press, 1973.-374 ń.
10. American Academy of Audiology. Clinical Practice Guidelines: Diagnosis, Treatment and Management of Children and Adults with Central Auditory Processing Disorder. August 2010. – 51 đ.
11. Law J., Boyle J., Harris F., Harkness A., Nye C. Prevalence and natural history of primary speech and language delay: Findings from a systematic review of the literature // International Journal of Language & Communication Disorders. 2000. Vol. 35, ą 2. pp.165-188.
12. Piaget J. et Inelder B. La psyuchologia de l’enfant. – Paris, 1966. – 576 p.
First Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The object of research in the presented work is disorders in children with ASD, the subject is actually the process of their diagnosis. The relevance of the study is undeniable, because, as the author himself rightly notes, "according to WHO data in the 2000s, every 61 children had a delay in speech development, now the data show that these developmental disorders are inherent in every 3rd child of preschool age. By school age, this figure stands at 25% in Russia and 19% abroad." The methodology is based on statistical analysis, which generally corresponds to the tasks stated in the text. The manuscript is executed in full compliance with the norms of scientific style, the author skillfully uses both general professional and highly specialized psychological and pedagogical terminology. The list of references in the bibliography corresponds to the content of the work. In the title, the word is written in English and, moreover, with an error (correctly - check-list), which looks frankly ridiculous. This word has already entered the Russian language in principle and is written in Cyrillic. On the other hand, in scientific language there are many ways of traditionally formulating the titles of articles with similar content "Features ...", "Specifics ....", "Varieties ....", therefore, the use of the "fashionable" word is completely unmotivated, despite the fact that scientific language is one of the most conservative by nature. Comments on this work are reduced to the understanding that, with an acceptable scientific and substantive quality in this form, it represents abstracts for publication in the collection of a practical conference, but not an article for a specialized scientific journal for the following reasons. 1) The text of the work without a bibliography contains about 8,000 pp. this is half the generally accepted lower threshold for a journal article. 2) The text completely lacks theoretical analysis. Elements of the theory, in particular a review of researchers at the level of a simple enumeration of surnames, are included in the introduction, similar to how it is done in theses. This is unacceptable for an article in a specialized publication. 3) There is a complete lack of description and justification of the methodology. The author simply names the method of work, while the journal article requires a more detailed explanation of why this particular toolkit was chosen, how this method is used and what tasks are solved with it. Usually the methodological part takes at least 1-2 full paragraphs. Note the qualitative description of the study sample. 4) The practical part of the article is made with partial compliance with the canons of the description of the psychological and pedagogical experiment. In fact, the author writes only about the diagnostic stage, while no formative and even more control work is carried out. In general, the presence of only one diagnosis may be acceptable for research in the format of an article, but in any case, the author should at least outline promising ways of working on its basis and explain exactly how the diagnosis led to an understanding of one or another practical aspect of the problem. This is the essence of experimental analysis, without which, in this presentation, the material has a reference form, but not a scientific and analytical one. So it is recommended to add a description of what exactly each violation manifests itself in. 5) There are no abstract conclusions in the article. If the author finally writes that "This checklist can be used for screening assessment of the spectrum of comorbid disorders in a child with speech retardation and to determine the direction of an in-depth examination in connection with the prevailing behavioral pattern," then it is reasonable to develop the idea and indicate these specific areas of further work. 6) In general, the focus solely on diagnostics extremely impoverishes the content of the text, since the methods of diagnostic work are standard and so well known to professionals working with children with ASD. A simple enumeration of violations and statistical data is difficult for a reader without relevant experience. This is not the way to talk about a full-fledged scientific novelty. 7) The article lacks the author's point of view, which in works with similar content, most likely, should be expressed in reflections on the effectiveness / inefficiency of certain methods of work, the reader is not invited to dialogue and reflection, which also distances the text from the journal format. All of the above characterizes the material as high-quality abstracts for a practical conference, or as a good professional report, but not a journal publication. It is recommended to expand this manuscript according to the above parameters in order to bring it to the format of a journal article. On the other hand, if the publication allows the publication of abstracts (as is practiced in exceptional cases by a number of journals), then the text can be published without revision. In the latter case, for formal compliance with a possible examination of the HAC, it is recommended to add "(abstracts based on the results of the study)" to the title.
Second Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The paper "Varieties of comorbid disorders in children with ASD" is presented for review. Every year there are more children with special health conditions. The subject of the study is the description of the types of comorbid disorders in children with ASD. The theoretical analysis carried out by the author revealed a contradiction between the need for diagnostic lists combining typical manifestations in psychological, pedagogical and psychiatric practice and their absence from specialists who work with this category of children. The advantage of the work is: 1). A large sample size – 1000 children aged 1.5 to 7 years, a long study period – from 2019-2022.. The author has compiled a program for the study of comorbid disorders, the main method of studying which is a retrospective analysis of maps. 2). The results obtained made it possible to identify neuropsychiatric manifestations and behavioral stereotypes of children with mental retardation. The work is characterized by a clear structure: an introduction with the definition of the purpose, methods, tasks, methodological basis; characteristics of the respondents; description of the results; discussion of the results. The prospects for further research have been determined. The work is written in scientific language, represents the author's contribution to solving the problem raised. The main recommendations are as follows: 1). To formalize the final section in the article – to draw a conclusion with structured and reasoned conclusions, substantiating the scientific significance and the author's contribution to solving the problem raised. 2). Based on the results obtained, it is necessary to develop a program or recommendations for working with such a category of children for specialized specialists. This, to a greater extent, will allow us to achieve the perspective indicated by the author – "we hope for the speech and intellectual development of this group of children, as well as the correction of these behavioral stereotypes by correcting their social communication and interaction skills", rather than just informing. 3). The bibliography of the article includes 12 domestic and foreign sources. The list contains a small number of publications dated over the past three years. The problems of the work correspond to the subject of the article. The bibliography contains scientific articles and several monographs. Most of the requirements are not met (for example, the number of sources is at least 20; 1/3 of the sources must be foreign, the date of publication, etc.). It is recommended to issue a bibliography strictly in accordance with the Rules for registration of literature 2022, posted in the section Rules for registration of the list of references. Taking into account the highlighted recommendations during revision will make it possible to submit a complete scientific work to the editorial board. The article is written in scientific language and is relevant from a theoretical point of view. The work is distinguished by its undoubted practical value. The article can be recommended for publication after correcting the comments.
|







