|
Psychology and Psychotechnics
Reference:
Nazmetdinova, D.G., Shamakov, V.A. (2023). Cross–cultural adaptation and approbation of the questionnaire "Stroke Self-efficacy Questionnaire" ("Self-efficacy after stroke"). Psychology and Psychotechnics, 3, 34–43. https://doi.org/10.7256/2454-0722.2023.3.40995
Cross–cultural adaptation and approbation of the questionnaire "Stroke Self-efficacy Questionnaire" ("Self-efficacy after stroke").
Nazmetdinova Dilara Gamzatovna
Postgraduate student, Senior Educator, Department of Genetic and Clinical Psychology, National Research Tomsk State University; Junior Scientific Associate, Department of Neurology, Tomsk Scientific Research Institute of Balneology and Physiotherapy branch of the Siberian Federal Scientific Clinical Center of Federal Medical and Biological Agency
634061, Russia, g. Tomsk, ul. Lebedeva, 8, kv. 173

|
dilara86@bk.ru
|
|
 |
Other publications by this author
|
|
|
Shamakov Viktor A
ORCID: 0000-0002-3716-7707
Researcher, Cognitive Research Laboratory, Faculty of Psychology, National Research Tomsk State University
634050, Russia, Tomsk region, Tomsk, Lenin Ave., 36
|
|
sva1.0@mail.ru
|
|
 |
|
DOI: 10.7256/2454-0722.2023.3.40995
EDN: FRGFWC
Received:
14-06-2023
Published:
22-06-2023
Abstract:
The article presents a step-by-step description of the procedure for cross-cultural adaptation of the questionnaire on the Russian sample. The goal is to adapt and test the Stroke Self-efficacy Questionnaire on stroke patients with an assessment of internal consistency and convergent validity. 77 patients of the Tomsk Regional Vascular Center filled out the Russian-language version of the "SSEQ" and the "Scale of general self-efficacy" (R. Schwarzer, M. Yerusalem, adapted by V.G. Romek) were studied. When filling out 13 scales of the questionnaire, patients assessed their abilities, capabilities, resources in performing everyday tasks after a stroke on a scale from 0 to 10, where 0 is absolutely not sure and 10 is absolutely sure. To assess convergent validity, post-stroke patients filled out a "Scale of general self-efficacy" consisting of 10 items, each of which has 4 degrees of consent of the respondent from "absolutely incorrect" to "absolutely true". The total values on the scale (from 10 to 40 points) reflect the overall indicator of subjective assessment of personal effectiveness. The article presents the psychometric characteristics of the test and descriptive statistics. The internal consistency of the test was determined by the Kronbach method. The coefficient is generally equal to 0.875. Adaptation and testing of the questionnaire "Self-efficacy after stroke" in many countries has shown good validity results. Cross-cultural adaptation of the questionnaire "Self-efficacy after stroke" was conducted in Russia for the first time. The advantages of using this questionnaire include the possibility of using it as an express technique in the work of a clinical psychologist within a multidisciplinary team to assess the motivational component of rehabilitation potential in the system of staged rehabilitation treatment.
Keywords:
stroke, cross cultural adaptation, self-efficacy, approbation of the methodology, ischemic stroke, rehabilitation, coefficient Cronbach, convergent validity, motivation, multidisciplinary team
This article is automatically translated.
Introduction According to WHO statistics, acute cerebral circulatory disorders still occupy a leading position worldwide due to a high increase in morbidity, mortality and impressive disability rates among the able–bodied population. According to the World Federation of Neurological Societies, at least 15 million acute disorders of cerebral circulation are registered annually in the world, and in Russia the incidence of hemorrhagic and ischemic stroke is more than 450,000 new cases per year, while currently there is a tendency to increase the incidence after Covid- 19 [1]. Modern research in the field of rehabilitation of post-stroke patients indicates a high probability of partial or complete restoration of lost functions as a result of early initiation of rehabilitation measures. Often, such events are generally focused on restoring physical health with the use of kinesotherapy, neuromuscular electrical stimulation, antithrombotic therapy, etc. [2,3]. In this context of medical rehabilitation, the patient takes the role of a passive participant in rehabilitation treatment, and the question of the formation of health-related behavior in him remains controversial. In turn, the analysis of the literature allows us to talk about the leading role of the patient's motivation for recovery, his independence, active involvement in the recovery process, which will determine not only the positive dynamics of treatment as a whole, but also preserves the long-term effect of rehabilitation [4]. Self-efficacy (a term proposed by A. Bandura) - confidence in their abilities to carry out the intended behavior can play an important role in increasing the motivation of patients (Bandura, 1986). At the same time, the better the patient evaluates his resources and opportunities for treatment, the more effort he will put to carry out the planned action, as much as possible to be involved in rehabilitation programs. For example, in one of the rehabilitation programs for patients suffering from arthritis, it was proposed to take a course of psychological intervention aimed at strengthening the perception of self-efficacy in overcoming difficulties. According to the results of the course, patients showed not only significant improvements in physical condition (reduction of pain, inflammatory processes), but also improved psychosocial functioning. The idea of self-efficacy, proposed in the late 70s of the XX century by Albert Bandura within the framework of socio-cognitive theory, became the conceptual basis for the creation of the "Stroke Self-efficacy Questionnaire" (abbreviated SSEQ) - a questionnaire of self-efficacy after a stroke [5]. For the first time, the questionnaire (SSEQ) was developed by the staff of the Faculty of Health and Social Protection and Education of the University of St. Petersburg.George (London, UK) in 2008 and has been successfully adapted in many countries to date: Denmark (2018), Turkey (2019), Portugal (2020). In Russia, adaptation and testing of the questionnaire "Self-efficacy after stroke" is carried out for the first time [6,7,8,9]. Methods The study involved 77 patients of the Regional Vascular Center at the Tomsk Regional Clinical Hospital: men (n= 33) and women (n = 44) aged 34 to 82 years. The inclusion criterion was the presence of the following diagnoses according to ICD - 10: I 63.0 - Cerebral infarction caused by thrombosis of the precerebral arteries; I 63.5 - Cerebral infarction caused by unspecified blockage or stenosis of the cerebral arteries, I 63.2 - Cerebral infarction caused by unspecified blockage or stenosis of the precerebral arteries; G 45.0 - vertebrobasilar arterial system syndrome; G 45.1 Carotid artery syndrome (hemispheric); G 45.9 - Transient cerebral ischemic attack, unspecified. The criteria for non-inclusion were the patient's refusal to participate in the study. The original questionnaire "Stroke Self-efficacy Questionnaire" is a list of 13 statements related to the daily activities that patients were engaged in before the violation of cerebral circulation. The task of the subjects was to assess their abilities in performing these tasks after a stroke on a scale from 0 to 10, where 0 is absolutely not sure and 10 is absolutely sure. Statistical procedures for processing the questionnaire were carried out using the R software package. The internal consistency of the Russian-language version of the SSEQ questionnaire was evaluated using the L. Kronbach formula. The convergent validity of the questionnaire was considered as a correlation of the self-efficacy scale with another method of measuring the same property, the so-called "gold standard". In this case, we used the "Scale of general self-efficacy" (R. Schwarzer, M. Yerusalem, adapted by V.G. Romek), consisting of 10 points, each of which has 4 degrees of consent of the respondent (from absolutely incorrect to absolutely true). The total values on the scale (from 10 to 40 points) reflect the overall indicator of subjective assessment of personal effectiveness [11]. Received data
The adaptation of the questionnaire "Stroke Self-efficacy Questionnaire" into Russian was carried out on the basis of international standards for translating the questionnaire into another language, which include several important points (Wild at al., 2005). At the initial stage, a written permission was received from one of the authors of the original SSEQ questionnaire, a professor at the Faculty of Health, Social Protection and Education of the University of St. Petersburg.George (London, UK) Fiona Jones for the translation and adaptation of SSEQ for Russian-language use.The next step was to carry out a direct translation of the questionnaire text from English to Russian with the most accurate transmission of the meaning of the questionnaire statements. For this purpose, the text was provided to 2 translators: an employee of the Faculty of Psychology at TSU, familiar with the concept of the questionnaire and a professional translator not from the field of medicine and psychology. At the approval stage, all discrepancies in translations were eliminated by making small changes to avoid too literal translation and to obtain semantic proximity with the original methodology. In order to identify the shortcomings of direct translation, a reverse translation from Russian to English was carried out. And finally, at the final stage of adaptation, independent experts (neurologists, medical psychologists) gave a positive assessment of the Russian version of the questionnaire. It is important to note that during the adaptation procedure, feedback from respondents for understanding questions, instructions, etc. was also taken into account. The questionnaire obtained during all the adaptation procedures was designated by us as R – SSEQ (R - Russian version). At the first stage, a sample analysis was carried out before assessing the internal consistency and convergent validity of the questionnaire. 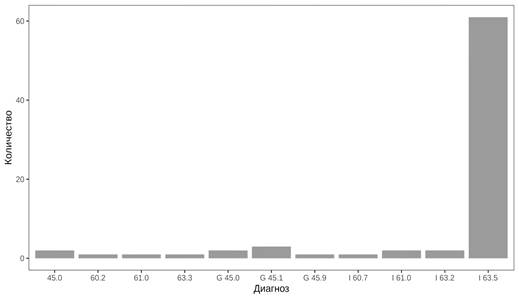
Fig. 1. Diagram of the ratio of the number of patients with cerebravascular diseases and diagnoses Figure 1 shows that the majority of the sample (n = 77 people) were patients with a diagnosis of I 63.5 - Cerebral infarction caused by unspecified blockage or stenosis of the cerebral arteries. In second place are patients with transient ischemic attack and related symptoms (ICD- 10 code: G 45.1 and G 45.0). This type of cerebral circulation disorder is similar to the symptoms of a stroke, but differs in episodic manifestations and blood circulation of the brain is restored in the first day. 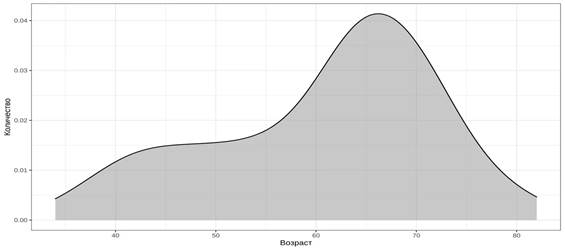
Fig. 2. Graph of the ratio of age and number of patients with cerebravascular diseases. In Figure 2 of the probability distribution density of the variable "age", it can be observed that the sample is for the most part normally distributed, although it has a slight orientation towards bimodality. In the left part of the graph, there is a noticeable trend towards the formation of a second group of younger patients. Interesting results were obtained when considering the variable "age" with division by gender (Figure 3): the distribution density for men begins to tend a little to symmetry, but the distribution density for women shows the very second group of young women affected by stroke. However, due to the small sample size, the results obtained are preliminary. 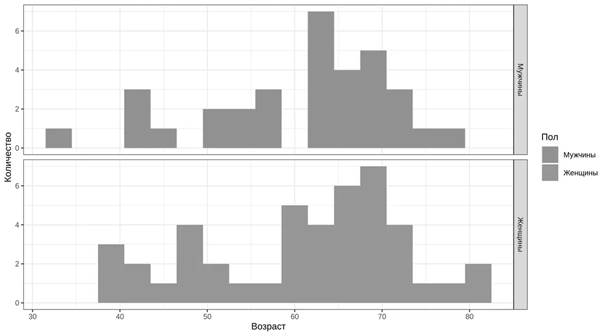
Fig.3. Diagram of the ratio of men and women by age (n =77) The indicator of internal consistency of the statements of the questionnaire was determined by calculating the Cronbach's ? coefficient using the formula: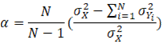 The standardized Cronbach 's alpha coefficient is calculated using the following formula: 
, where N is the number of components studied, and r determines the average correlation coefficient between the components With the minimum required value ? = 0.7, this indicator for the Russian version of the self-efficacy questionnaire after a stroke was 0.881. After the standardization procedure, the coefficient ? slightly increased to a value of 0.9.
The next stage of our research was the assessment of convergent validity using the questionnaire of "General Self-efficacy" ((R. Schwarzer, M. Yerusalem, adapted by V.G. Romek). As mentioned above, the total values on the scale of "General self-efficacy" range from 10 to 40 points, and in the questionnaire "Self-efficacy after stroke" - from 0 to 130 points, respectively. On the scattering diagram of the resulting variables of the SSEQ (self-efficacy after stroke) and GSES (General Self-efficacy Questionnaire) techniques, one can observe strongly declining values. 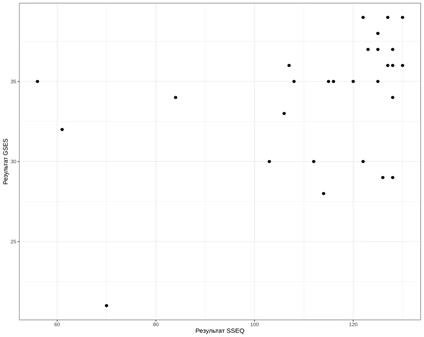
Fig. 4. Scatter diagram of the resulting variables of the SSEQ (self-efficacy after stroke) and GSES (questionnaire of general self-efficacy) techniques After a detailed analysis of the results of the questionnaires, contradictory responses of respondents to the questionnaire "Self-efficacy after stroke" were revealed. In the first case, the respondent indicated the inability to get out of bed on his own in the morning (statement No. 1) and do daily chores before the stroke (statement No. 12) and at the same time noted the ability to do current household chores for the highest 10th score (statement No. 4). In the second case, the subject noted in the responses high confidence to take a few steps around the apartment without assistance (statement No. 3) and absolute lack of confidence in his ability to go outside (statement No. 5). After deleting the data of the subjects from the general sample, the scattering diagram of the resulting variables of the SSEQ (self-efficacy after stroke) and GSES (questionnaire of general self-efficacy) methods acquired the following form (Fig.5) : 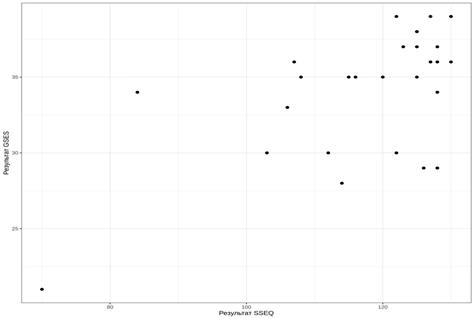
Fig. 5. The scattering diagram of the resulting variables of the SSEQ (self-efficacy after stroke) and GSES (questionnaire of general self-efficacy) techniques after the removal of "outliers" Discussion of the results The indicator of internal consistency of the statements of the questionnaire of the Russian—language version of the SSEQ questionnaire was determined by calculating the Cronbach's ? coefficient, which can take values from -? to 1, and a coefficient equal to 0.7 is considered a good value. The results obtained in the study (Cronbach's ? is 0.9) indicate a very good consistency of the questions among themselves and allow us to conclude that the validity of the Russian – the language version of the questionnaire "Self-efficacy after stroke". For comparison, the indicators of the Cronbach's ? coefficient in the adapted versions of the questionnaire in different countries were: in the original questionnaire – 0.9; in the Chinese version of the questionnaire – 0.92; in the Turkish version - 0.93, in the Portuguese version of the questionnaire the coefficient is 0.82. After removing 2 respondents with contradictory results from the total sample, the correlation coefficient between the resulting variables SSEQ (self-efficacy after stroke) and GSES (assessment of overall self-efficacy) at p-value 0.00008 was 0.6, while the Cronbach's alpha coefficient became 0.86. Which proves the convergent validity of the SSEQ-R questionnaire in the Russian sample. Conclusion The translation and cultural adaptation of SSEQ to the Russian version of "Self-efficacy after stroke" proved successful, with good reliability and internal consistency. The use of the test in the most practical way opens up wide opportunities both for diagnosis and for the development of rehabilitation treatment programs. The questionnaire can be used in the practice of a clinical psychologist as part of a multidisciplinary team in the diagnosis of the ICF – b 130 motivation domain. The use of the questionnaire "Self–efficacy after a stroke" at the late stages of rehabilitation (a year after a stroke) will allow the multidisciplinary team to determine the main difficulties of the patient after discharge from rehabilitation centers or during the transition "hospital - home", which will allow to adjust the program of rehabilitation treatment at the stage of the patient's stay in the rehabilitation center. The study was carried out with the support of the Russian Foundation for Basic Research,
project 19-313-90057 "Medical and psychological rehabilitation of patients with ischemic stroke
in the system of staged restorative treatment"
References
1. Voznyuk I.A., Ilyina O.M., & Komentsev S.V. (2020). Ischemic stroke as a clinical form and pathogenetic model in the structure of central nervous system lesions in COVID-19. Bulletin of Restorative Medicine, 4(98), 90-98. (In Russ.).
2. Miryutova N.F. (2015). Comprehensive rehabilitation of patients with consequences of acute cerebrovascular accident. Physiotherapy, balneology and rehabilitation, 1, 13-18. (In Russ.).
3. Ermakova N.G. (2018). Psychological rehabilitation of patients with the consequences of a stroke in conditions of rehabilitation treatment. Medical psychology in Russia, 2, 1-9. (In Russ.).
4. Rasskazova E.I., Tkhostov A.Sh., Kovyazina M.S., & Varako N.A. (2020). Changing the patient's lifestyle as a task of psychological rehabilitation: organizing rehabilitation as a joint activity at the personal and interpersonal levels. Clinical and Special Psychology, 1(9), 47–63. (In Russ.).
5. Schwarzer R., Yerusalem M., & Romek V. (1996). Russian version of the scale of general self-efficacy by R. Schwarzer and M. Yerusalem. Foreign Psychology, 7, 71-77. (In Russ.).
6. F. Jones, C. Partridge, F. Reid. (2008). The Stroke Self-Efficacy Questionnaire: measuring individual confidence in functional performance after stroke. The Authors. Journal compilation, 244-252. doi:10.1111/j.1365-2702.2008.02333.x
7. Lola Q. Kristensen, & H. Pallesen. (2018). Cross-cultural adaptation of the stroke self-efficacy questionnaire-Denmark (SSEQ-DK). Top Stroke Rehabilitation, 25(6), 403-409. doi:10.1080/10749357.2018.1469713
8. M. Makhoul, E. B. Pinto, N. A. Mazzini, C. Winstein, C. Torriani-Pasin. (2020). Translation and validation of the stroke self-efficacy questionnaire to a Portuguese version in stroke survivors ). Top Stroke Rehabilitation, 27(6), 462-472. doi:10.1080/10749357.2020.1713555
9. A. Gülcihan, A. Beser. (2019). Psychometric Testing of the Turkish Version of the Stroke Self-Efficacy Questionnaire. Journal of Nursing Research, 27(4), 35. doi:10.1097/jnr.0000000000000308
10. Schwarzer R., Yerusalem M., & Romek V. (1996). Russian version of the scale of general self-efficacy by R. Schwarzer and M. Yerusalem. Foreign psychology, 7, 71-77.
Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The work "Cross–cultural adaptation and approbation of the questionnaire "Stroke Self-efficacy Questionnaire" ("Self-efficacy after stroke") is presented for review. The subject of the study. The subject of the study is not indicated in the work. The work is devoted to the consideration of cross-cultural adaptation and approbation of the questionnaire indicated in the title of the article. In general, the article describes the theoretical and empirical aspects of its consideration. The results obtained may indicate that the subject has been studied in full. Research methodology. The study is based on the idea of self-efficacy, proposed in the late 70s of the XX century by Albert Bandura within the framework of socio-cognitive theory, which became the conceptual basis for the creation of the "Stroke Self-efficacy Questionnaire" (abbreviated SSEQ) - a questionnaire of self-efficacy after a stroke. The author conducted a study of 77 patients using the questionnaire "Stroke Self-efficacy Questionnaire" ("Self-efficacy after stroke"). The results obtained showed the presence of its effectiveness and high reliability. The relevance of the study is determined by the need for timely rehabilitation of post-stroke patients. This ensures a high probability of partial or complete restoration of lost functions as a result of early initiation of rehabilitation measures. At the same time, the patient should not take a passive position. The author's analysis of the literature will allow us to say about the leading role of the patient's motivation for recovery, his independence, active involvement in the recovery process, which will determine not only the positive dynamics of treatment as a whole, but also preserves the long-term effect of rehabilitation. Therefore, it is important to determine the self-efficacy of a patient after a stroke using valid and reliable psychodiagnostic tools. The scientific novelty of the study is as follows: tools were identified to consider the self-efficacy of patients after stroke, conclusions were drawn about successful testing, good reliability and internal consistency. Style, structure, content. The style of presentation corresponds to publications of this level. The language of the work is scientific. The structure of the work is clearly traced, the author highlights the main semantic parts. In a detailed introduction, the relevance is indicated, a brief theoretical analysis is given, and the main problem is identified. The main section is devoted to the description of the empirical research conducted and the analysis of the results obtained. The advantage of the work is to conduct a detailed data analysis. This allowed the author to highlight the main positions and discuss the results obtained. The article ends with brief conclusions. The work is a complete and complete work. Bibliography. The bibliography of the article includes 10 domestic and foreign sources, the number of publications over the past three years is not enough. The list contains mainly research articles and online sources. The sources are incorrectly designed. Appeal to opponents. Recommendations: 1) to make a deeper theoretical analysis, including modern, more recent sources; 2) to expand the conclusion, prescribing reasoned and more complete conclusions based on the results of the study, as well as the novelty and personal contribution of the author to solving the issues raised; 3) to concretize the prospects of this study, highlighting the main directions for further study; 4) to formalize correctly bibliographic list, bring it to uniformity in accordance with the requirements. Conclusions. The problems of the article are of undoubted relevance, theoretical and practical value, and will be of interest to specialists when conducting psychodiagnostic work. The article can be recommended for publication taking into account the highlighted recommendations.
|







